
En dynamisk rygg har dokumentert effekt på helse
Netti har signifikant klinisk bevis for følgende påstander:
En Netti dynamisk løsning vil kunne:
- Forbedre brukerens posisjon
- Redusere smerte og ubehag
- Redusere risikoen for trykksår
- Forebedre lunge kvalitet og redusere risikoen for lunge sykdommer
Disse påstander har kommet på plass etter en sammenligning mellom en statisk og en dynamisk rullestol.
There are several proven advantages of using the Netti dynamic back support
Improved position:
The Dynamic back solution will allow small as well as extreme upper body movements. Allowing these movements and supporting the user back in the original resting position when tone decreases, will help the user maintain the optimum seating position (1), prevent sliding (1) and shearing and lowering the need for repositioning. Especially for persons with muscular dysfunction, postural stability is essential to prevent spinal deformities as they have a higher incidence of scoliosis, lordosis, and kyphosis (2,3).
Reduced pain/discomfort:
Pain and discomfort will be reduced with a dynamic back support. There will be a significant reduction by more than 50 % of the peak forces on the back in the dynamic configuration compared to the rigid configuration (8).
A lower peak force has proven to result in less discomfort for the user. (9, 10)
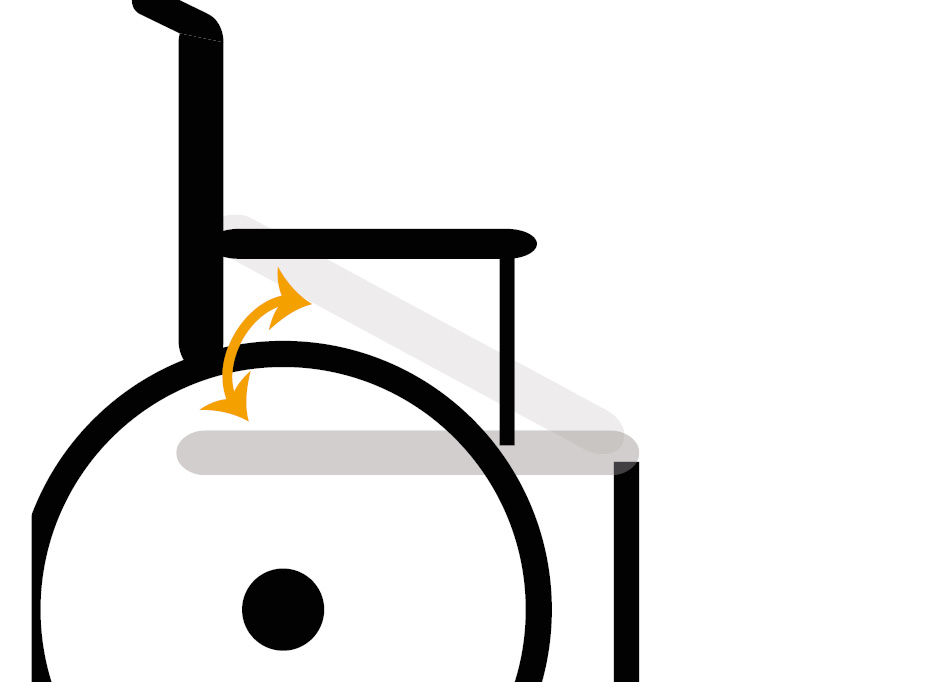
Reduced risk of decubitus / pressure sore:
It’s proven that a dynamic back support results in a significant better position and stability due to the user moving less in a downward direction while seated in the dynamic seating system (8).
Less pressure downward, relates to less tissue deformation. This is proved by a study by Ride Designs where it’s shown by MRI scans that the tissue is less deformed when the pressure is less (11)
Less tissue deformation is related to reduced decubitus ulcer (12)
To explain how low stability of trunk and pelvis is related to pressure ulcer can be explained via the proof from following studies: A pressure ulcer is localized injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear [13]. Remaining seated for extended periods of time increases the risk of pressure ulcers development over the buttocks, as the soft tissue in this area is squashed between two surfaces: the seat and the bones of the pelvis (14, 15, 16). How long this destruction to the skin takes can often be irrelevant as some pressure ulcers develop quickly and others take longer (17).
The process is dependent on other factors such as health status, disability, ability to change position, and maintaining an upright-seated position without slumping or sliding (17).
A key study [18]found that when sitting naturally, only a small amount of pressure for one to two hours could lead to the development of a pressure ulcer as body weight in this position, is redistributed over a smaller area [19]resulting in high pressures in the buttocks [20, 21]. This extra pressure upsets the blood flow through the skin starving the area of oxygen and nutrients, and if this goes unrelieved begins to break down, leading to the development of a pressure ulcer. To help understand the severity of damage to the skin from pressure, an international pressure ulcer staging system is used (22). The higher the stage the more severe the pressure ulcer and damage to the skin and underlying tissues.
Improved lung health:
As sliding down is limited, it in turn, prevents sitting in a slumped posture. A slumped posture is associated with a decreased lung capacity. Hence, the lung function will be better while using a dynamic system (4)
Being able to move from a seating to an almost supine position has its influences on many body parts and functions. One of the parts is the diaphragm and its function which is breathing. The study “Diaphragmatic motion in the sitting and supine positions” (5) has shown that the diaphragms mobility in supine is higher than in sit.
The diaphragm is the primary muscle of respiration, and its weakness can lead to respiratory failure. A larger excursion of the diaphragm means a deeper and more functional breathing where all areas /parts of the lungs are used, better circulation is maintained, and chances of infections are reduced (6, 7).
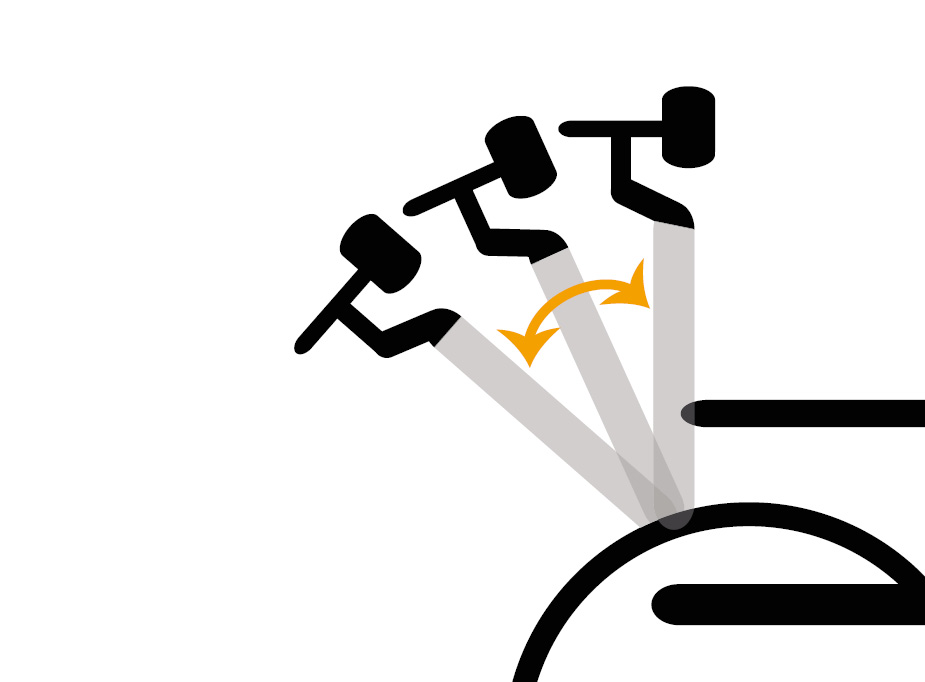
Dynamic back support
The Dynamic back solution will allow small as well as extreme upper body movements. Allowing these movements and supporting the user back in the original resting position when tone decreases, will help the user maintain the optimum seating position, prevent sliding and shearing and lowering the need for repositioning. Our flexible back solution comes in 2 different types.
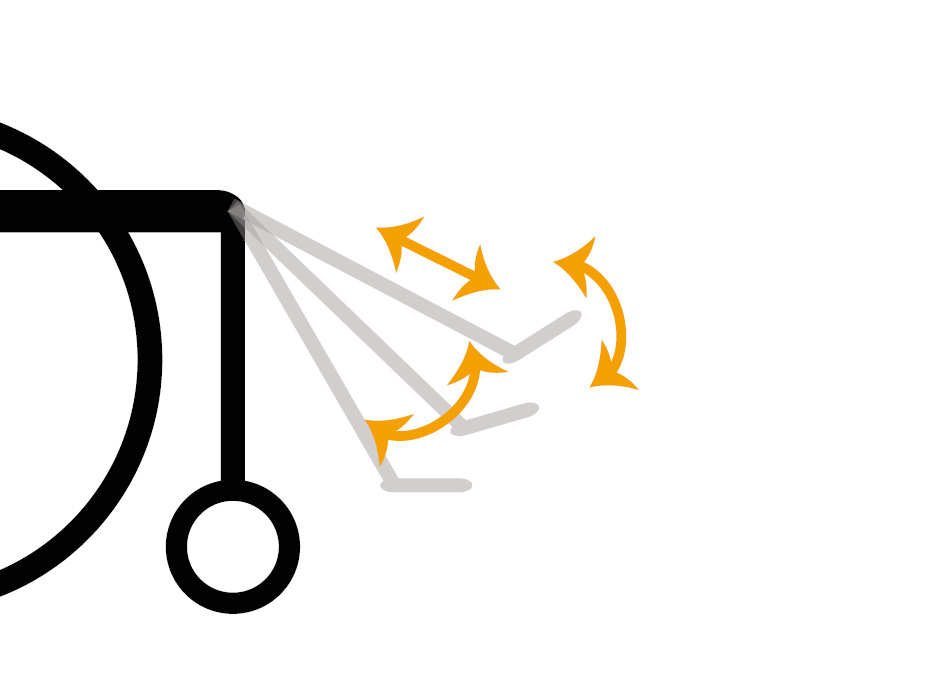
When extreme upper body movements are the challenge, the dynamic back support needs to be assisted with dynamic seat plate, hip belt as well as leg supports.
Related articles


Reference list:
1. Cimolin V, Piccinini L, Avellis M, et al. 3D-
Quantitative evaluation of a rigid seating system and dynamic seating system using 3D movement analysis in individuals with dystonic tetraparesis. Disabil Rehabil Assist Technol. 2009;4(6):422-428. doi:10.3109/17483100903254553
2. Hong E-K, Dicianno BE, Pearlman J, Cooper R, Cooper RA. Comfort and stability of wheelchair backrests according to the TAWC (tool for assessing wheelchair discomfort). Disabil Rehabil Assist Technol. 2016;11(3):223-227. doi:10.3109/17483107.2014.938365
3. Samuelsson K, Bjork M, Erdugan A-M, Hansson A-K, Rustner B. The effect of shaped wheelchair cushion and lumbar supports on under-seat pressure, comfort, and pelvic rotation. Disabil Rehabil Assist Technol. 2009;4(5):329-336. doi:10.1080/17483100902978426
4. Lin F, Parthasarathy S, Taylor SJ, Pucci D, Hendrix RW, Makhsous M. Effect of different sitting postures on lung capacity, expiratory flow, and lumbar lordosis. Arch Phys Med Rehabil. 2006;87(4):504-509.doi:10.1016/j.apmr.2005.11.031
5. Diaphragmatic motion in the sitting and supine positions, Healthy subject study using a vertically open magnetic resonance system Ryutaro Takazakura MD, Masashi Takahashi MD , Norihisa Nitta MD, Kiyoshi Murata MD
6. Diaphragmatic dysfunction
7. Ricoy, N. Rodríguez-Núñez, J.M. Álvarez-Dobaño, M.E. Toubes, V. Riveiro, L. Valdés
8. : Identifying decreased diaphragmatic mobility and diaphragm thickening in interstitial lung disease: the utility of ultrasound imaging Pauliane Vieira Santana, Elena Prina, André Luis Pereira Albuquerque, Carlos Roberto Ribeiro Carvalho, Pedro Caruso, J Bras Pneumol. 2016 Mar-Apr; 42(2): 88–94
3D-Quantitative evaluation of a rigid seating system and dynamic seating system using 3D movement analysis in individuals with dystonic tetra paresis, Disability and Rehabilitation: Assistive Technology, 4:6, 422-428, DOI: 10.3109/17483100903254553
By: Veronica Cimolin, Luigi Piccinini, Martino Avellis, Andrea Cazzaniga, Anna Carla Turconi, Marcello Crivellini & Manuela Galli
9 Variability of peak shoulder force during wheelchair propulsion in manual wheelchair users with and without shoulder pain, Y.Moon, C.Jayaraman, I.M.K.Hsu, I.M.Rice, E.T.Hsiao-Wecksler, J.J.Sosnoff
10. Advances in Physical Ergonomics and Human Factors”. Proceedings of the AHFE 2017 International Conference on Physical Ergonomics and Human Factors, July 17-21, 2017, The Westin Bonaventure Hotel, Los Angeles, California, USA
11. Off Loading Wheelchair Cushion Provides Best Case Reduction in Tissue Deformation as Indicated by MRI Evan Call , Thomas Hetzel , Chad McLean , Joshua N Burton , Craig , Oberg
12. Deformation of tissues has been shown to be a greater indicator of pressure ulcer formation than pressure exerted on tissues alone”
Coleman S, Nixon J, Keen J, et al. A new pressure ulcer conceptual framework. J Adv Nurs 2014;70:2222–2234
13. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance Emily Haesler (Ed.), Prevention and treatment of pressure ulcers: quick reference guide, Cambridge Media, Osborne Park, Australia (2014)
14. Wounds UK Expert Working Group: International review. Pressure ulcer prevention: pressure, shear, friction and microclimate in context. A consensus document Wounds International, London (2010)
15. T.A. Krouskop: A synthesis of the factors that contribute to pressure sore formation Med Hypothesis, 11 (2) (1983), pp. 255-267
16. V. Schubert, J. Héraud The effects of pressure and shear on skin microcirculation in elderly stroke patients lying in supine or semi-recumbent positions Age Ageing, 23 (5) (1994), pp. 405-410
17. A. Gefen: How much time does it take to get a pressure ulcer? Integrated evidence from human, animal, and in vitro studies Ostomy Wound Manag, 54 (10) (2008), pp. 26-28, 30-35
18. M. Kosiak: Etiology and pathology of ischemic ulcers Arch Phys Med Rehabil, 40 (2) (1959), pp. 62-69
19. A.M. Cook, J. Miller Polgar: Cook and Hussey’s assistive technologies: principles and practice (third ed.), Mosby, London (2007)
10. J.C. Barbanel: Pressure management Prosthetics Orthot Int, 15 (1991), pp. 225-231
21. T. Defloor, M.H. Grypdonck: Sitting posture and prevention of pressure ulcers Appl Nurs Res, 12 (3) (1999), pp. 136-142
22. European Pressure Ulcer Advisory Panel, National Pressure Ulcer Advisory Panel & the Pan Pacific Pressure Injury Alliance: Prevention and treatment of pressure ulcers: quick reference guide (2014)